







Wildlife casualties in general practice
Wildlife casualties are a common presentation to veterinary practices, usually brought in having been found by a member of the public. In this article, Vicki Baldrey, lecturer in exotic species and small mammal medicine and surgery at the Royal Veterinary College in London, discusses the approach to the wildlife casualty in a general practice setting and describes some of the most common presentations seen
Click on image to view




The aim of wildlife casualty treatment is to release the animal back into the wild in a fully fit state, as rapidly as possible, without compromising its welfare.1 Considerations for the animal include stress when hospitalised in an unfamiliar environment, the proximity of potential predators, the duration of captivity and the time of year. Considerations for the vet include a perceived lack of knowledge or experience, a lack of appropriate facilities or equipment, and time and financial pressures. Most wildlife casualties occur as a direct or indirect result of human actions and the public have expectations that we will do our best to look after any animal regardless of species. Working with injured wildlife can be a fascinating change from more routine cases, and hugely rewarding.
Legislation
Under section 23(6) the Wildlife Act 1976-2012, the Minister may grant a licence to a person to have in possession for a reasonable period of time an injured or disabled protected wild animal, or one or more than one dependant young of a protected wild animal, which is orphaned with the intention of tending and later releasing such animal or young back into the wild when and only when such animal is no longer injured, disabled or dependant. Its subsequent release is then subject to the conditions set out in the licence provided for the possession/retention of the animal. The licence is issued by the National Parks and Wildlife Service (NPWS). Three commonly encountered species are not protected by this legislation: the red fox, rabbit and grey squirrel. A licence is, therefore, not required for these species, although it is important to note the grey squirrel is classed as an invasive species and as such its release is not permitted. The Animal Health and Welfare Act 2013 ensures animal’s needs are met in captivity and protects them from unnecessary suffering. This legislation applies to all species.
Under the Veterinary Practice Act 2005 vets have a duty of care to provide emergency care or euthanasia to any species of animal to relive suffering, this includes providing emergency care out of hours. It does not require the treatment to be provided free of charge.
Triage
Wildlife casualties often arrive without warning, with limited clinical history. Essential information to be obtained when a wildlife casualty is presented includes:
• Exactly when and where animal was found;
• Any history of trauma or obvious clues for cause of injury;
• Any treatment or food given so far; and
• Contact details of the finder.
It is useful to have a standard form kept at the reception desk for the person presenting the animal to fill out. This ensures no details are missed. Triage should be performed immediately, and emergency treatment provided without delay, to avoid unnecessary suffering. These cases are all too often left until the end of clinics or even the end of the day without appropriate care.
Firstly, the species must be identified. A useful website to assist with identification is www.conserveireland.com. Correct identification is vital to ensure an appropriate plan for housing, diet and medications can be made. Time should then be spent on hands-off observation – what is the demeanour of the animal, any signs of respiratory distress, obvious injuries or postural deficits, eg. head tilt, lameness. It is crucial to know what is normal for the species, in particular the behaviour, ecology, seasonality, feeding behaviour and breeding status.
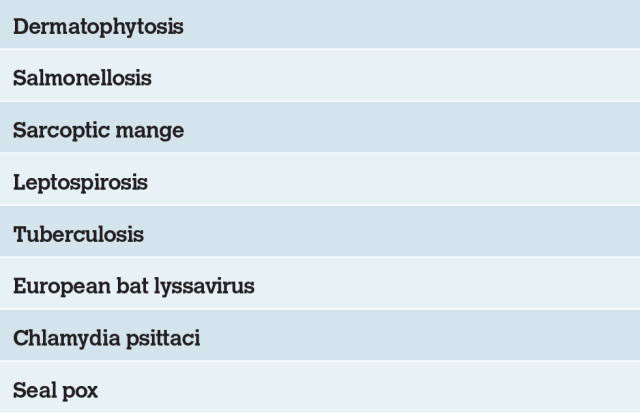
Before handling, ensure all necessary equipment and medications are prepared to minimise repeated capture and restraint. For more fractious species it is helpful to have an assistant. Appropriate personal protective equipment (PPE) should be used. Table 1 lists the most common zoonotic diseases associated with wildlife casualties. For small mammals a crush cage may be used to enable injection with a sedative to allow a full clinical examination. For birds a towel may suffice to facilitate handling.
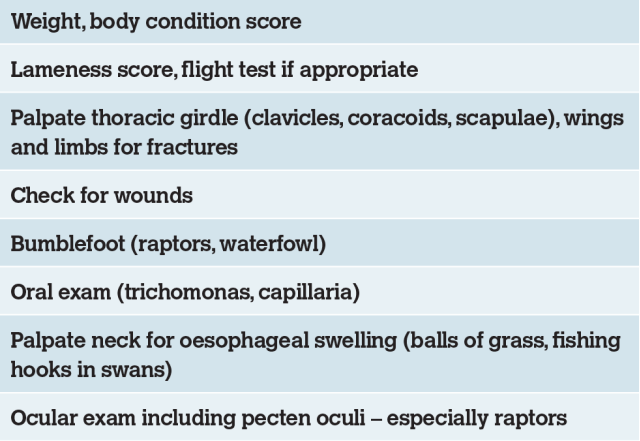
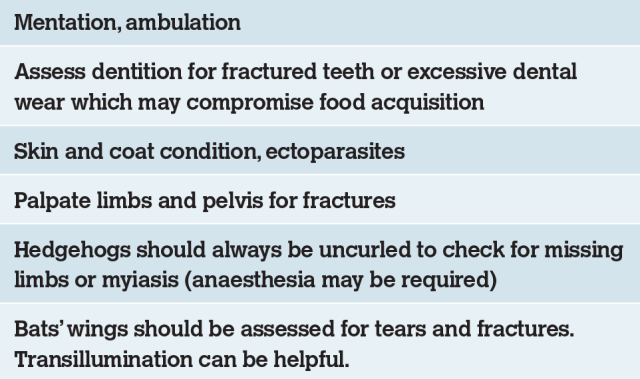
Initial triage should establish the urgency of treatment, assess whether treatment or rehabilitation are required and whether release is likely. To be suitable for release an animal must have an equal chance of survival to its wild conspecifics. If this is not realistic then euthanasia at an early stage is the best option for the welfare of the individual. Initial examination should assess vital signs, body condition score and any obvious wounds or injuries. Tables 2 and 3 outline the important features of the avian and mammalian clinical examination. Age may be estimated by feathering, gape and dentition.
Nestling birds are partially feathered and gape for food (Figure 1), fledglings are fully feathered and don’t gape.
The outcome of the initial examination may be:
• Immediate release – this is rarely appropriate. Most cases will benefit from observation for at least 24 hours. Exceptions include entanglement and misguided rescue attempts, for example fledgling birds. In many species, fledglings are fed on the ground prior to their flight feathers becoming fully grown and these birds should be returned to the site they were found without delay, or preferably not removed at all;
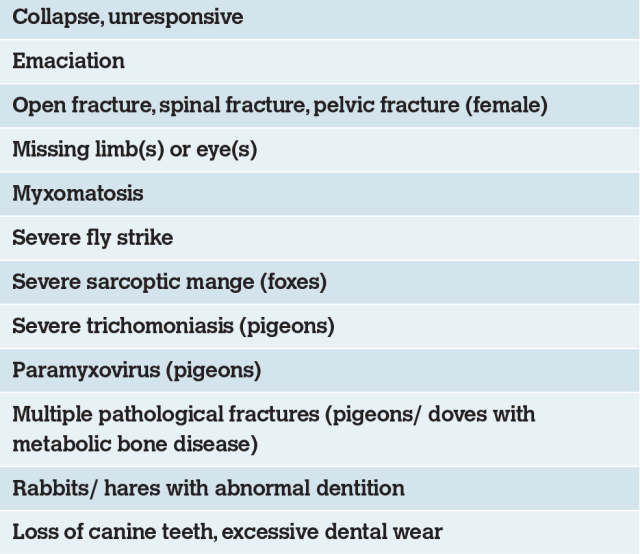
• Immediate euthanasia. This can be controversial. An early decision is important to minimise stress and suffering. If in doubt reassess frequently and discuss with a colleague or rehabilitator. Table 4 lists the most common reasons for immediate euthanasia.
• Treatment and rehabilitation leading to release.
Euthanasia techniques for birds include intravenous pentobarbitone into the right jugular, medial tarsal or cutaneous ulna vein, or intrahepatic pentobarbitone. If using the intrahepatic route, it is essential to ensure the liver is pierced and the injection is not given into the air sac. Wherever possible the intravenous route should be used to avoid this risk. Euthanasia techniques for mammals include intravenous pentobarbitone via the jugular, cephalic or marginal ear vein (rabbits). Under anaesthesia the cranial vena cava may be accessed, or alternatively the intracardiac route may be used. Before considering further treatment, it is important to consider the following questions:
• Do I have the facilities to hospitalise this animal without undue stress?
• Do I have the facilities and expertise to manage this case (eg. complicated fracture)?
• Is there a very good likelihood of future release?
If the answer to any of the above questions is no, the animal should be transferred to a wildlife rehabilitator or euthanasia performed on welfare grounds.
Hospitalisation
A team approach to these cases is vital and veterinary nurses play a very important role as the main caregivers while these animals are in clinics. Accommodation should be quiet and secure and away from the sight, scent and noise of predators. It should be easy to observe the animal discreetly and to change the food and water without undue disturbance. Enclosures must be easy to clean between patients. Appropriate perching should be provided for avian patients and a tail guard applied to all raptors to prevent feather damage (Figure 2). A rolled-up towel can be formed into a donut shape to support to protect the keel if the bird is recumbent.
Stabilising of the wildlife casualty
-
Oxygen, if required.
-
Warmth. Wildlife casualties are often hypothermic on presentation and active warming is required. This is also essential for juvenile animals. Heat sources include microwave heat pads, hot water bottles, thermostatically controlled heat pads and overhead radiant heat bulbs. Whatever source is used, the animal must be able to move away from direct contact and must not be able to damage it by chewing.
-
Analgesia. This is vital as many wildlife casualties will be suffering from traumatic injuries. Opioids are used for moderate to severe pain. Buprenorphine or methadone are suitable for mammalian species, however avian species possess mainly kappa receptors so butorphanol is a more suitable choice for these species. Non-steroidal anti-inflammatory drugs (NSAIDs) are also suitable for most species once hydration is corrected. An up to date formulary should be consulted for doses.
-
Fluids. Intravenous fluid administration may not be well tolerated by larger mammal species, however, can be very useful for larger birds such as waterfowl. If IV access is not a suitable choice, then subcutaneous fluids may be used alongside oral fluids. Hyaluronidase can be added to subcutaneous fluids at a dose of 1,500IU per litre to increase speed of absorption. Fluids should be warmed to body temperature prior to use.
-
Nutrition. A variety of food choices should be offered and should mimic the natural diet as closely as possible. Time of day should be considered, for example nocturnal species such as hedgehogs should be fed in the early evening. Crop tubing or syringe feeding with an appropriate critical care formula is required if the patient is not self-feeding.
Common case presentations
Hedgehogs
Hedgehogs are solitary nocturnal insectivores. They produce four to five hoglets per litter from late spring until early autumn and orphaned animals are not uncommon during this time. Hedgehogs hibernate from January to March and must be over 650g in weight and in good body condition prior to release to ensure enough body reserves to survive this period.2 Being out during the day indicates a problem (apart from pregnant or nursing females who may forage during daylight hours) and further investigation is indicated.
Common problems include trauma, often caused by strimmers, dog bites, road traffic accidents (RTAs); myiasis, dermatophytosis associated with Trichophyton erinacei and lungworm caused by Crenosoma striatum and/or Capillaria aerophila. The treatment of choice for lungworm is levamisole, although follow up treatment with ivermectin may be required in some cases.3 Severe cases require antibiotics for secondary bacterial infection, NSAIDs and mucolytics. Nebulisation can also be helpful. Dermatophytosis may be treated with oral itraconazole or terbinafine. Terbinafine has been shown to be superior in one study.4 Care must be taken to decontaminate the environment as this infection is highly contagious.
Hogs should be housed in a secure container with a hide area. Shredded paper is ideal for bedding. A suitable diet in captivity includes wet dog food with dry food available to reduce tartar formation. If anorexic, then syringe feed with a commercial carnivore critical care diet can be performed.
Foxes
Foxes live in family group in an earth. They are primarily nocturnal, and their natural diet includes voles, rabbits, birds, fruit and carrion. They breed in January/February with cubs usually born in late March. Problems include trauma, usually from road traffic accidents (RTAs), gunshot injuries, snare injuries or bite wounds from conspecifics. Fractures may be managed in the same was as in domestic dogs, however consideration should be given to the number of interventions and length of captivity required as this is stressful for adults and may result in tameness in younger cubs.5 Infectious diseases include canine distemper, hepatitis and leptospirosis and euthanasia is recommended for these cases. Sarcoptic mange is common and can be treated with ivermectin or selamectin, however advanced cases often have concurrent problems and euthanasia may be required.6 Tame foxes are unreleasable and housing juveniles outdoors in social groups helps to avoid this. Foxes can be hospitalised in a dog kennel with the door covered with a towel to reduce stress. For longer-term housing an outdoor run is preferred. Short-term diet can be canned or dried dog food, but this should be supplemented with rats, mice, day old chicks and pieces of rabbit in the longer term.
Badgers
RTAs are very common, leading to traumatic injuries and fractures. These may be managed in the same way as foxes, with the same potential complications. Snare wounds are common and often lead to pressure necrosis and deep wounds that can take a few days to become apparent. Dentition should be carefully evaluated as excessive wear is common in geriatric badgers and these will not be able to acquire enough food to survive. Rump wounds are common following territorial disputes. Badger cubs must have three negative blood samples for TB before they may be released. Some rehabilitation centres vaccinate adult badgers prior to release, although this is not a legal requirement.
Pigeons and doves
Feral and racing pigeons tend to be very calm and can be restrained in the traditional pigeon fancier’s grip. In contrast, woodpigeons are loose feathered and tend to flap excessively when handled. A towel and two-handed grip should be used, to avoid excessive feather loss.
Trauma is common and especially fractures of the wing or thoracic girdle. If just the radius or ulna is fractured, then a simple figure of eight bandage is appropriate (Figure 3). Fractures of the clavicle, coracoid or scapula require a figure of eight bandage that is extended to wrap around the body and immobilise the shoulder joint. The bandage should be removed every five to seven days to allow passive range of motion physiotherapy to prevent restriction of joint mobility.
Metabolic bone disease is frequently seen in juvenile wood pigeons and collared doves and leads to folding fractures which can be detected on radiographs. These birds should be supplemented with calcium and vitamin D, and UVB light provided during captivity.
Trichomoniasis (canker) is extremely common, causing caseous lesions in the mouth, pharynx and crop. Flagellates may be seen on wet preparations from the mouth or crop. The disease can be treated with metronidazole or carnidazole if not too advanced, however severe cases should be euthanased. As many birds are asymptomatic carriers and the disease is highly contagious, some authors recommend routine treatment of all incoming Columbiformes with a single dose of carnidazole.7
Pigeon paramyxovirus causes head tremors, torticollis (Figure 4), ataxia and watery droppings. An asymptomatic carrier state is possible. Birds can theoretically recover with six to eight weeks of supportive treatment, but euthanasia is advised due to the contagious nature of the virus.
Waterfowl
Swans, ducks and geese may be kept in a walk-in kennel short-term, with the door covered with a towel. They should be fed greens soaked in water or ideally waterfowl pellets. They may be gavage fed with a herbivore critical care recovery formula if not eating. Botulism is common in summertime and tends to affect mainly swans and gulls. It is caused by the ingestion of toxin from the Clostridium botulinum bacterium and usually occurs during the summer months. Treatment is supportive care with fluids, tube feeding and nursing care. Mildly affected cases can recover with supportive treatment; however, the prognosis is poor if clinical signs are severe.
Lead toxicosis affects swans following ingestion of lead, mainly from fishing litter. Affected swans present with muscular weakness leading to a kinked neck (limber neck). Ingested lead is visible on a gizzard X-ray, however the absence of lead does not rule out toxicity and blood lead levels are required. Treatment is sodium calciumedetate 25-40mg/kg subcutaneously once daily for five days on, two days off, five days on, repeated until clinical signs have resolved.8 A gizzard flush is straightforward if necessary and follow up radiographs will demonstrate success.
Exposure to hooks and fishing litter is also common and swans may be presented with fishing line hanging from the beak. In this case, radiographs should be taken of the neck and body to identify a hook if present. If no hook is present then the line can be removed with gentle traction, which is often easier under anaesthesia. If a hook is present in the oesophagus it can be surgically removed, however if in the proventriculus then surgical removal is more challenging. Hooks in the gizzard can usually be left to degrade and grind down.
Passerines
Cat bite injuries are common and should always be considered serious. Infection with Pasteurella multocida is a common sequel so treatment with broad spectrum antibiotics (amoxicillin is a good first line choice) is essential, even if a puncture wound is not immediately visible.9 Analgesia and treatment of shock is also necessary. It is important to remember that damaged feathers will not regrow until the next moult so this should be considered when planning rehabilitation.
Summary
Wildlife casualties are commonly presented to vets in general practice and should be triaged without delay. An understanding of basic biology and physiology of the commonly presented species is necessary for the veterinary surgeon to provide appropriate emergency care and make decisions regarding the chances of successful rehabilitation and release. If release is unlikely or the period in captivity will be prolonged, consideration must be given to euthanasia on welfare grounds.
Author
Vicki Baldrey BVSc BSc(Hons) DZooMed(Avian) FHEA MRCVS, lecturer in Exotic Species and Small Mammal Medicine and Surgery, Beaumont Sainsbury Animal Hospital, Royal Veterinary College, London.
Further resources
- Wildlife Rehabilitation Ireland, www.wri.ie – rehabilitation resources and Wildlife
- Veterinary Treatment courses for veterinary nurses and veterinary surgeons.
- Irish Wildlife Matters – www.irishwildlifematters.ie – first aid, rehabilitation and treatment resources and species-specific veterinary pages covering common conditions, treatment and drugs and dosages tables.
- BSAVA Manual of Wildlife Casualties
- Lafeber vet – https://lafeber.com/vet/
- Wildpro – http://wildpro.twycrosszoo.org
- https://www.avma.org/KB/Policies/Documents/euthanasia.pdf – describes species specific euthanasia techniques.
- Meredith A. Wildlife triage and decision-making. In: BSAVA Manual of Wildlife Casualties: British Small Animal Veterinary Association; 2016.
- Bunnell T. The Assessment of British Hedgehog (Erinaceus europaeus) Casualties on Arrival and Determination of Optimum Release Weights Using a New Index. Journal of Wildlife Rehabilitation 2002; 25(4): 11-21.
- Bexton S, Couper D. Veterinary care of free-living hedgehogs. In Practice 2019; 41(9):420-32.
- Bexton S, Nelson H. Comparison of two systemic antifungal agents, itraconazole and terbinafine, for the treatment of dermatophytosis in European hedgehogs (Erinaceus europaeus). Vet Dermatol. 2016; 27(6): 500-504.
- Couper D, Bexton S. Veterinary treatment of fox casualties. In Practice 2016;38(3):130-8.
- Couper D. Foxes. In: BSAVA Manual of Wildlife Casualties: British Small Animal Veterinary Association; 2016.
- Chitty J. Pigeons and doves. In: BSAVA Manual of Wildlife Casualties: British Small Animal Veterinary Association; 2016.
- Goulden S. Waterfowl. In: BSAVA Manual of Wildlife Casualties: British Small Animal Veterinary Association; 2016.
- Lawson B, Best D. Passerines and other small birds. In: BSAVA Manual of Wildlife Casualties: British Small Animal Veterinary Association; 2016.
1. For which of the following species is a rehabilitation licence not required?
a. Red fox
B. Badger
C. Mallard
D. Swift
2. Which of the following would be the most suitable method of humane euthanasia for a collapsed mute swan with an open fracture of the humerus?
a. Intrahepatic pentobarbitone
B. Intracoelomic pentobarbitone
C. Intravenous pentobarbitone delivered via the medial tarsal vein
D. Intracardiac pentobarbitone
3. A mute swan presents in late winter with muscle weakness and limber neck. What is the most likely diagnosis?
a. Botulism
B. Lead poisoning
C. Pasteurella infection
D. Trauma
4. What is the most likely complication of a cat bite in a juvenile blackbird?
a. Septicaemia due to pasteurellosis
B. Septicaemia due to salmonellosis
C. Trichomoniasis
D. Avian pox virus
5. Which of the following is a common zoonotic infection of the European hedgehog?
a. Sarcoptic mange
B. Chlamydia psittaci
C. Mycobacterium bovis
D. Trichophyton erinacei
Answers: 1:A; 2:C; 3:B; 4:A; 5:D.