Preventing and managing dermatophytosis in the equine hospital
It is very important to fully understand the aetiology and pathogenesis of dermatophytosis to effectively prevent its spread within the equine hospital, writes Sarah Meub, Crowe’s Veterinary Clinic, Carrick-on-Shannon, and final-year veterinary nursing student at Dundalk Institute of Technology
Dermatophytosis or ‘ringworm’ is a common fungal infection of the superficial layers of the skin and hair (Holtgrew-Bohling, 2016). Although it doesn’t pose major health risks to horses, unlike many other infectious diseases seen in practice, ringworm is highly contagious and can be zoonotic. Veterinary nurses (VNs) play important roles in the management of infectious diseases, such as performing diagnostic tests, advising clients, and ensuring excellent hygiene protocols are designed and implemented in the practice (Payne, 2009).
Suspected cases of ringworm should be placed in isolation immediately and barrier nursed until a definitive diagnosis is reached. Ringworm can often present subclinical and concurrent to other pathological issues. This increases the risk of transmission, as the horse may be presented for simple diagnostic procedures, such as limb radiographs, which do not warrant close inspection or isolation, allowing the horse to shed fungal spores throughout the practice. As equine practices tend to be very busy, subtle skin lesions may be overlooked if strict examination and hygiene protocols are not followed.
Pathogenesis
Once a horse is infected, the incubation period typically ranges from seven to 14 days, but can take up to four weeks for any clinical signs to appear (Dillon, 2014). Dermatophyte fungi are highly contagious, but the disease tends to be self-limiting (Sullivan, 2015), and cases usually resolve in one to three months (Coumbe, 2001). By this time, the fungal spores can spread far and wide in the environment, therefore, treatment is advised.
Dermatophytes are spread by direct contact or via fomites such as tack, grooming equipment, clothing, etc. This makes accidental cross-contamination of patients extremely easy if veterinary staff don’t remain vigilant. A case of undetected ringworm can spread infective spores throughout the practice, potentially infecting other patients, and people. Although equine dermatophytes affect humans less commonly than dermatophytes associated with dogs, cats, and livestock, there remains a significant zoonotic potential.
The main concern is that the fungus can persist in the environment for up to 12 months causing infection long after the initial case (Holtgrew-Bohling, 2016). This means that meticulous cleaning and disinfecting of all areas in contact with the horse are vital to prevent further spread.
Economic implications of ringworm outbreaks in equine practice
Outbreaks of infectious diseases such as ringworm can lead to serious economical and legal implications (Swain, 2003). It can severely taint the reputation of the practice if horses return having acquired a nosocomial infection. Horses affected by ringworm are prohibited to attend horse races (BHA 2019), shows, or sales. The Irish Horseracing Regulatory Board (IHRB) has similar powers to disqualify infected horses from racecourses (Dillon 2014). Horses may also be prohibited from traveling abroad. This results in financial losses for the client. Vets are obliged to disclose potential ringworm infections when completing veterinary soundness certificates; if the presence of a ringworm infection is overlooked, it can leave the veterinary practitioner and the entire practice in a legally vulnerable position (Dillon, 2014).
Aetiology and clinical signs
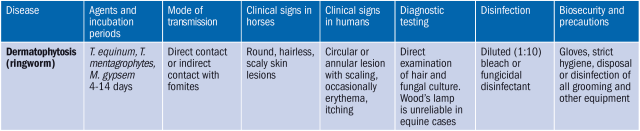
The causative agents of importance in equine practice are Microsporum gypsem, Trichophyton equinum, and Trichophyton mentagrophytes (Caveney et al, 2012). Ringworm can affect horses of all ages but is most commonly seen in horses under three years of age, older horses, and immunocompromised individuals (Dillon, 2014). This emphasises the risk of spread in the equine practice as many of our patients have concurrent illnesses and, therefore, are more susceptible.
When examining each horse, special attention should be paid to typical predilection sites for ringworm. Lesions can occur anywhere on the body but are predominantly seen in the girth and saddle areas, as well as the face, eyes, and legs (Dillon, 2014). See Figure 1.
Ringworm in horses may be mildly pruritic, but much less so than in small animal cases (Coumbe, 2001). In the early stages of infection, small tufts of hair appear raised, bumpy, and urticarial (White, 2005). As the disease progresses, the hair covering the infected areas is lost revealing raised, circular lesions, which appear grey and flaky (Sullivan, 2015). See Figure 2. The hair around the periphery of each lesion appears broken and rough (Coumbe, 2001). The lesions range in size from 2mm to over 5cm in diameter depending on the stage of infection (Dillon, 2014).
Sample collection
Samples are generally collected as hair plucks from the periphery of active, non-medicated lesions (White, 2005). Always apply disposable gloves before collecting samples due to the zoonotic risk. Wipe the area with 70% isopropyl alcohol to reduce contamination of the sample. Allow the area to dry and pluck a few of the broken hairs along with the skin scales from the edge of the lesion using a sterile forceps and place in a sterile, labelled container (Coumbe, 2001).
Diagnostic tests
Ringworm is generally diagnosed via fungal culture and/or microscopic examination. For fungal culture, the sample may be plated onto Sabouraud’s dextrose agar and incubated at 37°C. This will promote the growth of fungal colonies, which can then be examined microscopically for a definitive result (Sirois, 2015).
Standard dermatophyte test media (DTM) may also be used. DTM is a form of modified Sabouraud’s dextrose agar that contains the pH indicator dye, phenol red, which changes colour if dermatophyte growth occurs (White, 2005).
The disadvantage of fungal culture is that it requires specialised equipment, such as an incubator and specific test media. This may not be feasible for smaller practices to perform in-house, requiring the assistance external laboratories. Fungal culture is also not very efficient as it can take up to 10 days for results (Dillon, 2014), and negative results are not always reliable (Coumbe, 2001). Also, Trichophyton verrucosum does not grow on DTM, indicating further analysis of the sample even if the test yields a negative result (White, 2005).
Alternatively, microscopic examination offers a quick and cheap option for analysing samples in-house and requires minimal equipment. The procedure for a microscopic examination is outlined below.
A Wood’s lamp is also commonly used to aid diagnosis of ringworm as some strains are fluorescent under ultraviolet light (Dillon, 2014). Although this method is commonly used in small animal practice, it can be unreliable as many dermatophyte species affecting horses do not fluoresce and will result in a false negative (Holtgrew-Bohling, 2016).
Microscopic examination
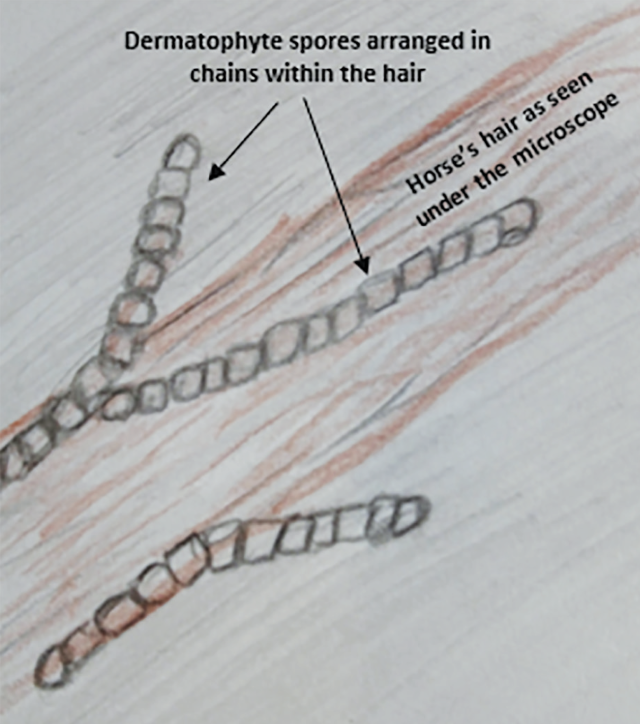
Place some of the hair pluck onto a glass slide, add one to two drops of 10% potassium hydroxide and apply a cover slip to the slide. Warm the slide gently by placing over a radiator for two to 10 minutes and examine the sample under a microscope. Additionally, a Romanowski stain such as Diff-QuiK or gram stain (fungal components will stain blue) may be used to enhance the visibility of fungal morphology if necessary (Caveney et al, 2012).
Upon examination, a sample of hairs infected by dermatophyte fungi appear frayed and distorted under low-power magnification. Examination under high power will show characteristic fungal hyphae and arthrospores attached to the hair shafts (Patterson & Ball, 2013). See Figure 3.
Biosecurity and biocontainment of dermatophytosis
Biosecurity is defined as ‘all the cumulative measures that can or should be taken to keep disease from occurring and prevent the transmission of disease. The policies and hygienic practices designed to prevent incidents of infectious disease.’ (Caveney et al, 2012).
This is a key area for VNs to fulfil in practice. There are many different levels of biosecurity needed for various diseases, some being of much higher infectious risk than others. In the case of ringworm, the risk of transmission through environmental fomites is high but the disease itself is self-limiting and non-fatal. Therefore, effective barrier nursing techniques, along with appropriate cleaning and disinfecting, are sufficient control measures.
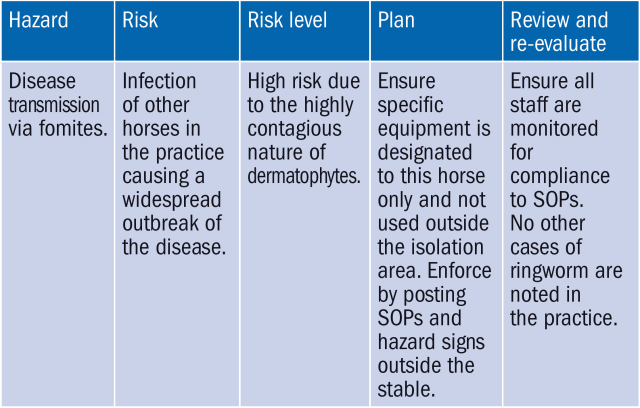
The risk assessment
In order to control contagious diseases, standard operating procedures (SOPs) should be written up specific to each condition. These include plans, protocols, procedures, and policies that are essential to disease management. This is done by conducting a risk assessment of the situation to identify the hazards and potential risks of the disease. From there, a plan can be devised on how to prevent transmission. A copy of the completed risk-assessment and disease-control plan should be clearly posted at the entrance to the isolation unit or area (see Table 2).
Isolation protocols
Once a horse is suspected to be infected with ringworm, appropriate actions must be taken immediately at admission. Ideally, the horse should be placed in a designated isolation facility for further examination and diagnostic testing (Swain, 2003). This should preferably be a building located a distance from the main hospital. The area should be stocked with a full range of veterinary equipment, cleaning equipment, and various disposable personal protective equipment (PPE) (Swain, 2003). Segregation of the patient and the use of strict hygiene protocols is generally sufficient to control ringworm. An important consideration when housing patients with ringworm is that the stable should have no porous or wooden surfaces that can harbour dermatophyte spores (Holtgrew-Bohling, 2016).
Barrier nursing
Effective barrier nursing involves isolating the patient in a stable, which can be done in conjunction to a dedicated isolation unit or within the general stabling area. It essentially creates a ‘barrier’ between the infectious horse, the nursing staff, and other patients (Monsey & Devaney, 2011).
In order to set up a barrier nursing stable, an area in front of the stable should be clearly demarcated with tape and signs to advise people of the risks and precautions necessary when handling the horse. No staff or personnel should enter this area without appropriate personal protective equipment (PPE [Swain, 2003]).
Personnel
Once the barrier area is set up, the infected horse should be treated last during daily rounds (Monsey & Devaney, 2011). This enables personnel to care for the horse without inadvertently infecting other horses and allows time to change out of any PPE, place disposable items in appropriate bins and clean and disinfect equipment before continuing to other tasks. It can be very easy to forget to wash your hands and disinfect your boots before continuing to the next stable, increasing the risk of transmission via fomites (Swain, 2003).
Recommended PPE for handling ringworm patients includes disposable gloves; waterproof wellies or boots; and hair covers. These should be worn by all people in contact with the horse. Dedicated clothing or disposable overalls should be worn when handling the horse and removed and left inside the isolation or barrier area (AAEP 2012). Once treatment of the horse is complete, remove all disposable PPE and place into appropriate clinical waste bins.
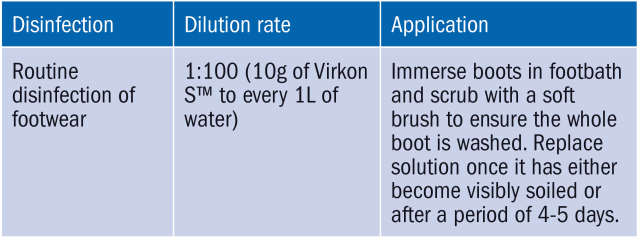
To disinfect boots, footbaths must be located at the entrance of the barrier area. Staff should be instructed to use the footbaths every time the isolation area is exited (Sheridan, 2009). Multi-purpose disinfectant agents, such as Virkon S™, are commonly used in large animal practice as they are highly effective in controlling a range of pathogens, including dermatophytes (Lanxess, 2019). See Table 3 for instructions for use.
Routine hand hygiene is a core factor in reducing the spread of infection (Forrest, 2007). Hand washing facilities must be available within the isolation area ie. warm running water, antiseptic hand soap, disposable paper towels and alcohol hand rubs. All personnel must wash their hands after handling the horse or any related equipment, regardless of the use of disposable gloves (Forrest, 2007). VNs should reinforce strict hand hygiene protocols in isolation areas by staying vigilant towards colleagues and acting as good role models.
Cleaning and disinfection
Cleaning and disinfecting all surfaces and equipment that have come in contact with the horse are some of the most important steps when it comes to the biocontainment of ringworm, since the disease is predominantly spread by fomites (Dillon, 2014). Environmental disinfectants should be selected appropriate to the disease and the product used as per manufacturer’s guidelines regarding dilution, contact time, etc. (Sheridan, 2009). A broad-spectrum disinfectant (such as Anistel™ surface disinfectant) may be used in ringworm cases for both equipment and environmental disinfection (Tristel, 2019). A 1:40 bleach and water solution may also be used to treat the environment (Holtgrew-Bohling, 2016).
Equipment
Any reusable equipment, headcollars, ropes, buckets, etc. should be thoroughly cleaned to remove any organic matter and soaked in a suitable fungicidal disinfectant solution such as Anistel or Virkon S for 20 minutes. Feed and water buckets should be rinsed thoroughly after applying the disinfectant.
Reusable barrier clothing, horse rugs, and other washable items should be soaked in 1:100 Anistel solution for 20 minutes and machine washed at over 60°C to ensure all spores are destroyed. Any equipment used when cleaning the area must also be disinfected, such as yard brushes, pitchforks, and wheelbarrows.
Stable environment
There should be specific disinfection SOPs in place for the housing of infectious cases. This should include step-by-step instructions to effectively remove all spores from the environment, eliminating the risk of transmission onto future patients. Please see sample SOP below.
- Remove any loose fittings such as buckets etc.
- Remove all bedding and organic matter from the stall. Manure can be disposed into the general muck heap, provided it is well maintained and turned regularly.
- Alternatively, used bedding can be placed in clinical waste bags.
- Wet all surfaces with a low power hose and remove all organic matter using a suitable detergent solution and a hard bristle scrubbing brush.
- Rinse all surfaces thoroughly with clean water.
- Apply a suitable fungicidal disinfectant to all surfaces using a trigger spray bottle and leave for the recommended contact time.
- Allow the disinfectant to dry without rinsing and repeat if necessary.
If possible, allow the stall to dry fully and remain empty for a few days before re-bedding. - Environmental swabs can be collected and submitted for fungal culture to ensure all spores are removed successfully.
The VNs role in treatment
Once ringworm has been diagnosed, veterinary practitioners will usually prescribe topical treatment of the lesions. It often becomes the VN’s role to ensure treatment is administered correctly.
Most cases respond well to enilconazole washes (Sullivan, 2015) such as Imaverol™. This topical treatment is generally safe and can be used on all horses regardless of pregnancy or illness. The solution is prepared 1:50 with tepid water. Soak any crusts over the lesions with the prepared solution and gently remove using a stiff bristled brush. It is advised that the entire animal should be sprayed with the solution in order to reach subclinical lesions at first treatment (Merial, 2019). Some horses have a strong dislike for the sound of a trigger-spray, making this part of the treatment rather difficult. In this case you may consider spraying the solution onto a clean sponge or cloth before entering the stable and then rubbing the horse down with the solution instead. The dermatophyte lesions and surrounding skin are then washed with the solution four times at three-day intervals (Merial, 2019). The solution is allowed to dry without rinsing.
Research has shown that tea tree oil (TTO) is also proven to be an effective fungicidal agent against dermatophytes (Pisseri et al, 2009). A study published in the International Journal of Phytotherapy and Phytopharmacology tested two groups of 30 horses infected with ringworm. They were treated with a mixture composed of 25% TTO in sweet almond oil, and enilconazole washes respectively for 15 days. After 30 days all horses were tested for dermatophytes and showed complete clinical healing (Pisseri et al, 2009). This mixture can be recreated by combining 100% pure TTO and sweet almond oil at a ratio of 1:3. Both ingredients are readily available for purchase in most health stores and pharmacies within Ireland and the UK (ie. Holland and Barrett, Evergreen.ie, Boots, etc.).
This method of treatment may be of interest for clients who may be deterred by the cost or who prefer a holistic approach to treatment. A benefit is that treatment can begin immediately if ringworm is suspected, but a definitive diagnosis has not yet been reached (Pisseri et al, 2009).
Client advice
In cases where the infection has not fully cleared or the horse is only admitted for a short time, the responsibility of treating the infection will fall to the client. VNs must be able to advise the client on how to apply the prescribed medication, as well as cleaning and disinfecting their own premises in order to manage infection and prevent transmission. Below are a few points that should be emphasised when offering advice on the treatment and prevention of ringworm.
Wear disposable gloves when handling the horse until the infection has cleared.
Do not use grooming equipment, tack etc. from this horse on other horses.
Keep the horse in a separate stall or field and avoid direct contact with other horses until the infection has cleared.
It is beneficial to let the horse out on sunny days, as the ultraviolet light from bright sunlight can help kill the spores (Dillon, 2014).
Clean and disinfect all in-contact surfaces and items with a 1:40 diluted bleach and water solution i.e. stables, grooming equipment, gates, saddles, etc.
Inspect all in-contact horses for signs of ringworm infection.
Avoid moving the horse onto other premises until the infection is cleared.
Wash hands frequently when handling infected horses.
Conclusion
Although ringworm is a very common skin disease in horses, it is highly contagious with the potential to cause major outbreaks. It is important that VNs are able to identify clinical signs early and act accordingly to prevent transmission to other patients. Optimal hygiene standards must be maintained and re-evaluated frequently to ensure the effective biocontainment of infectious diseases. VNs must have good knowledge of the disease processes in order to select appropriate interventions and implement hygiene protocols specific to the care of individual patients.
- American Association of Equine Practitioners. Biosecurity guidelines [online]. 2012. Available from: https://aaep.org/sites/default/files/Guidelines/BiosecurityGuidelinesFinal1.pdf [accessed 08 March 2019].
- British Horseracing Authority. The rules of racing [online]. 2019. Available from: http://rules.britishhorseracing.com/Orders-and-rules&staticID=126615&depth=3 [accessed 09 March 2019].
- British Small Animal Veterinary Association. Health and safety [online]. 2019. Available from: https://www.bsava.com/Resources/Veterinary-resources/Medicines-Guide/Health-and-safety-in-the-dispensary [accessed 09 March 2019].
- Caveney L, Jones B and Ellis K. Veterinary Infection Prevention and Control. Chichester: Wiley-Blackwell. 2012.
- Corley K and Stephen J. The Equine Hospital Manual. Oxford: Wiley-Blackwell Publishing; 2008: 186.
- Coumbe K. Equine Veterinary Nursing Manual. Oxford: Wiley-Blackwell; 2001: 256-277.
- Dillon, H. Ringworm in Horses. Veterinary Ireland Journal 2012; 4(7): 363-366.
- Forrest N. Controlling the spread of infection in the veterinary practice. Veterinary Nursing Journal 2007; 22(2): 14-15.
- Holtgrew-Bohling K. Large Animal Clinical Procedures for Veterinary Technicians. 3rd ed. St. Louis: Elsevier. 2016.
- Lanxess. Virkon: Disinfectant foot dip preparation and use [online]. 2019. Available from: http://virkon.com/products-applications/disinfectants/virkon-s/how-to-use-virkon-s/disinfectant-foot-dips/ [accessed 08 March 2018].
- Merial Animal Health. Summary of product characteristics: Imaverol [online]. 2019. Available from: http://www.hpra.ie/img/uploaded/swedocuments/Licence_VPA10481-001-001_18022019150914.pdf [accessed 08 March 2019].
- Monsey L and Devaney J. Maintaining animal accommodation. In: Cooper, B. et al., eds. BSAVA Textbook of Veterinary Nursing. 5th ed. Gloucester: BSAVA 2011: 297-303.
- Patterson S and Ball C. A practical approach to equine dermatology. In Practice 2013: 35(4) 190-196.
- Payne L. The role of the dermatology nurse. Veterinary nursing journal 2009; 24(5), 47-49.
- Pisseri F, Bertoli A, Nardoni S et al. Antifungal activity of tea tree oil from Melaleuca alternifolia against Trichophyton equinum: an in vivo assay. Phytomedicine: International Journal of Phytotherapy And Phytopharmacology 2009:16(11) 1056-1058.
- Sheridan L. Considerations for isolation and barrier nursing. Veterinary Nursing Journal 2009: 24(3) 12-14.
- Sirois M. Laboratory Procedures for Veterinary Technicians. 6th ed. St. Louis: Elsevier. 2015: 274-275.
- Swain J. Isolation protocols in the equine hospital. Veterinary Nursing Journal 2003: 18(6) 184-187.
- Sullivan S. Summer seasonal skin conditions of the horse. Veterinary Ireland Journal 2015: 5(7) 323-324.
- Tristel. Anistel surface disinfectant [online]. 2019. Available from: http://www.tristel.com/anistel-products/anistel-surface-disinfectant [accessed 08 March 2018].
- White S. Equine bacterial and fungal diseases: A diagnostic and therapeutic update. Clinical Techniques in Equine practice 2005: 4(4) 302-310.