







Hedgehogs – a practical approach to common presentations
Aoife Hand MVB O’Malley Veterinary Hospital, Bray, aims to equip general practitioners with the tools to appropriately triage and treat hedgehogs without compromising their welfare
The European hedgehog (Erinaceus europaeus), or ‘gráinneog’ in Irish, is one of Ireland’s most beloved, and commonly encountered native wildlife species. While the hedgehog is protected by Irish law under Wildlife Acts 1976-2012, as well as the Bern Convention Appendix III, it is still one of the most frequently presented wildlife casualties in Irish veterinary practice. This is mainly due to the many anthropogenic hazards associated with coexisting alongside humans.
Hedgehogs are solitary insectivores, inhabiting sheltered hedgerows, fields and urban gardens. Due to a likely abundance of resources and food, hedgehogs are not known to be territorial.8 Their primary natural predators are badgers, however the majority of hedgehog casualties seen in practice are associated with human contact. Adult hedgehogs typically weigh 800-1,000g. They live for, on average, two to three years. Their characteristic features are their dorsal keratin spines, which enable them to evade predators when tightly rolled into a ball using their orbicularis muscle. They are a nocturnal species, with only pregnant or nursing females venturing out to forage during the day. They hibernate during the winter months but will wake intermittently during warmer weather. Breeding occurs from late spring through to early autumn.
Triage
An immediate and thorough clinical exam is integral when approaching hedgehog casualties. It is important that the extent of illness/injury be assessed as soon as possible to begin appropriate treatment, or if necessary, to humanely euthanise without delay. It is important to keep in mind that the International Wildlife Rehabilitation Council (IWRC) defines wildlife rehabilitation as: ‘The treatment and temporary care of injured, diseased, and displaced indigenous animals and the subsequent release of healthy animals to appropriate habitats in the wild’.7 This should be at the forefront of your mind when examining any wildlife case presented to you. If the likelihood of successful release and survival in the wild is slim, then it is imperative that the hedgehog be humanely euthanised immediately to prevent any further suffering. Hedgehogs that are deemed unfit for release into the wild should never be kept as household pets, as this significantly compromises their welfare as a wild animal. A basic step-by-step approach to the clinical examination of a wild hedgehog is described in Table 1.

Figure 1: Hedgehog with ringworm.
It is important to wear gloves when handling hedgehogs, as they are common, asymptomatic carriers of dermatophytes (Trichophyton erinacei). Even when ringworm lesions are not clinically apparent, the risk of zoonosis is still present. As many hedgehogs become stressed while in captivity, all efforts should be made to reduce stress when handling. Observe in a quiet area, away from other hospital patients. To unroll the hedgehog, gently rock, stroking their spines in a craniocaudal direction. Avoid touching the head or face. Once they have been unrolled, elevate the hindlegs carefully, so that the hedgehog is in a wheelbarrow position, with their front limbs resting firmly on a non-slip surface. From this position the hedgehog can be examined fully. Sex is determined by the greater anogenital distance seen in males versus females. The average temperature of a hedgehog is 33.5-36.8°C. Resting heart rate sits at 200-280 beats per minute, with 20-25 breaths per minute. If the patient is stable and not dehydrated or hypothermic, anaesthesia can be used to enable you to perform ancillary diagnostics and procedures too stressful to complete while the hedgehog is awake. Gaseous anaesthesia using isoflurane is recommended for both induction and maintenance of anaesthesia as injectable agents have a higher risk of overdose and prolonged anaesthetic effects. Always attempt to complete as much of your physical exam as possible, in the conscious patient.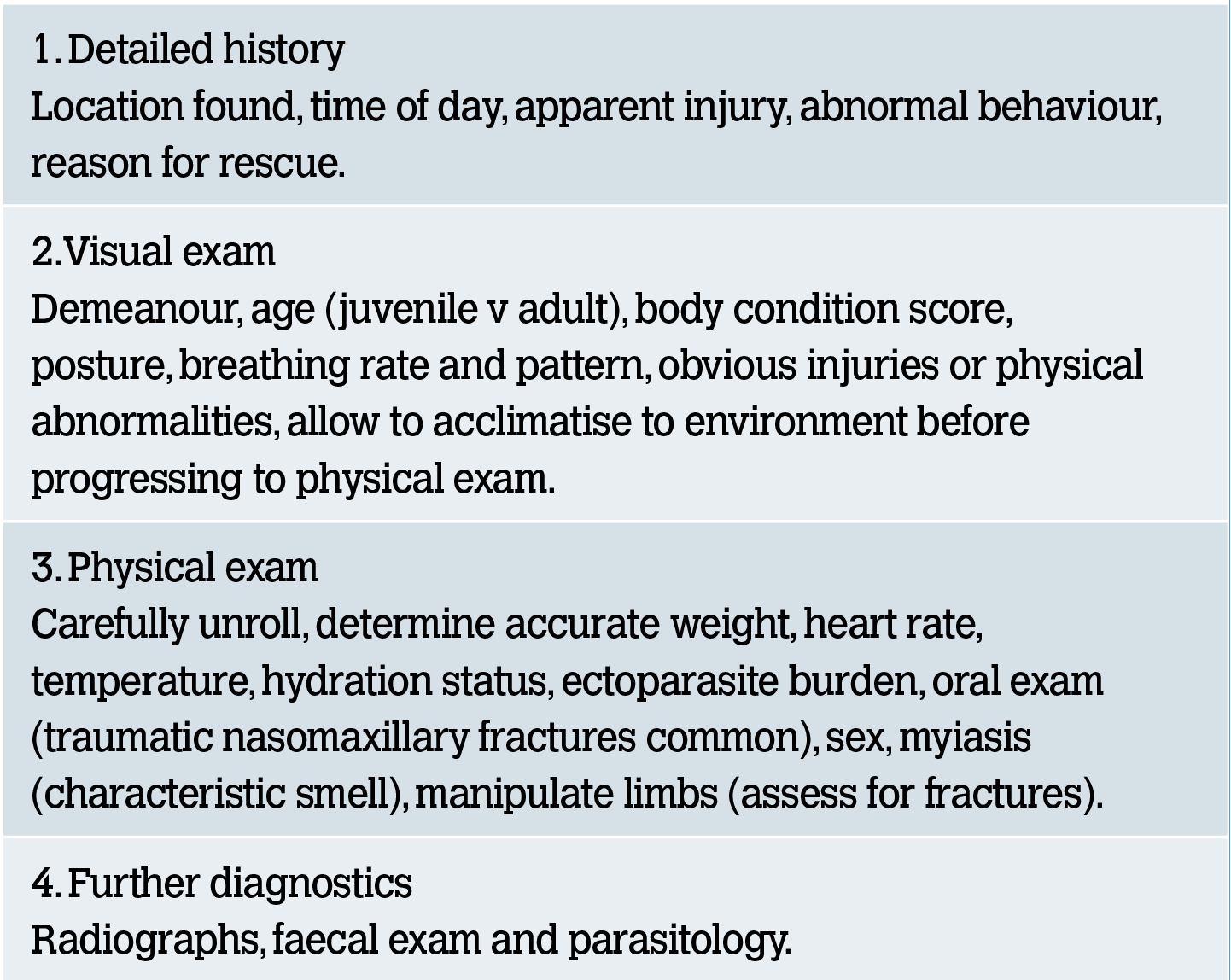
Table 1: Basic hedgehog clinical exam.
Husbandry and nutrition
Often when hedgehogs are brought into your clinic, they are found underweight, dehydrated and hypothermic. Hypovolaemia may even be present following trauma. It is important that you prioritise warming the hedgehog slowly using a heat pad (always allow the hedgehog to escape the heat source if needed). Subcutaneous fluid administration is the most effective means of rehydration in hedgehogs. Lifting the skin along the dorsum and injecting sterile crystalloid fluids at multiple sites is recommended.

Figure 2: Hypothermic hedgehog being warmed.
Housing hogs in your clinic may be required on a temporary basis until a suitable rehabilitator has been located. During this time, you should house the hedgehog in an isolation kennel or cat carrier. Try to avoid wooden boxes as they are difficult to sterilise between patients. Open-topped kennels pose the risk of an unwanted in-clinic escapade. Shredded paper is ideal as bedding, and should be changed on a daily basis. Hiding spots should be provided to allow the hedgehog to escape stressful situations and feel more at ease in their environment. Supplementary heat should be provided as needed, but again, always allowing the opportunity for the hedgehog to move away from the heat source. To minimise stress, all wildlife inpatients should be kept in a separate room, away from all other domestic animals in the clinic.

Figure 3: A hog in a captive habitat.
While food and water should be available at all times, feeding should occur in the evening to emulate the hog’s natural feeding behaviour. It is impractical to provide a complete insect diet in captivity, so wet and dry cat/dog food is a suitable short-term substitute. Including the dry food is important if the hedgehog is to be kept in captivity for an extended period of time, as dental tartar is a common side effect of a purely wet diet.5 Anorexic animals should be syringe-fed until eating independently.
Unfortunately, it is not uncommon for young hoglets to be rescued and brought into your practice following the death of their mother. While prolonged care and rearing of these juveniles will likely be done by a trained rehabilitator, it is important for practitioners to know how to examine and care for these youngsters on presentation. Newborns should be kept at an ambient temperature of 25-30°C. Once warmed, they should be given oral rehydration fluid, followed by canine/feline milk replacer fed via a small teat – 2ml of milk replacer given per feeding (every two to three hours) is sufficient for most newborn and young hoglets.9 They require anogenital stimulation to void, and typically produce green faeces while milk fed. From about four weeks of age, most hoglets should be able to lap milk independently. At this time, you can start to introduce a small amount of wet puppy/kitten food mixed into the milk. It is important that the hoglets are weighed daily to ensure that adequate nutrition is being provided. Bloat and milk aspiration are common problems in hand-reared hoglets.9 These can be avoided by maintaining a consistent feeding routine. Hand-reared hoglets have poorly developed immune systems due to a lack of maternal antibodies, and strict hygiene and barrier nursing should be maintained.
Common presentations
Trauma: Many hedgehogs seen in practice will be brought in following trauma: road traffic accidents, dog bites, strimmer injuries, burns etc. Wound management is the same as with other mammalian species, but it is important to remember that myiasis is common, especially in older wounds, and should always be investigated. A course of broad-spectrum antimicrobials (potentiated amoxicillin) is often required as secondary infection and abscessation is common. Reserve enrofloxacin for use only in refractory cases, as a second line antibiotic based on culture and sensitivity. Fracture repair should only be attempted if the prognosis of return to normal function following splint placement or surgical repair is good. Any animals with comminuted fractures or facial fractures, compromising their ability to breathe or eat effectively, should be euthanised on welfare grounds. Spinal injuries can be diagnosed by the flattening of all dorsal spines caudal to the point of injury. It is important to repeat your physical exam on a daily basis as the full extent of injuries may not always be immediately apparent.

Figure 4. Hedgehog with mandibular fracture.
Autumn juveniles: Juvenile animals, born later in the year, are at the greatest risk of being underweight at the onset of hibernation. Unlike nursing sows, when these juveniles are spotted out in daylight, they look dazed, malnourished, and often have large parasite burdens. While different sources suggest different optimal hibernation weights, it is generally accepted that hedgehogs found in the winter months that are <450g should be rescued and taken into captivity. They should be given anthelmintic treatment and unless sufficient weight gain is reached, should be kept in captivity throughout the winter months. Captive hedgehogs should not be released until they are >650g to optimise survival.4 It is, however, important to prevent obesity in hedgehogs during prolonged captivity as this can lead to an inability to effectively roll, thus hindering their survival. For this reason, it is recommended that hedgehogs be kept at a body weight of <1kg while in captivity.
Parasites: The most common endoparasite of concern in hedgehogs, especially in debilitated autumn juveniles, is lungworm (Crenosoma striatum or Capillaria aerophila). A distinct moist cough is often present in infected individuals. Faecal screening is recommended for diagnosis, but not always possible, and prophylactic treatment in the autumn and winter months is advised. Levamisole at 20-30mg/kg SQ every 48 hours, for three injections is the treatment of choice.2 Concurrent antibiotic therapy and anti-inflammatories can be used to treat secondary infections, and reduce airway inflammation and the risk of anaphylaxis, respectively. If treatment with levamisole is unsuccessful, follow up with ivermectin as needed. Intestinal capillariasis is also common, with green mucoid diarrhoea seen with heavy parasitic burdens. Table 2 shows the therapeutic agents efficacious in treating these conditions.

Figure 5. Hedgehog with mild tick burden.
Hedgehogs with significant ectoparasite burdens are usually affected by a primary condition, resulting in reduced grooming behaviour and a compromised immune system. This allows previously controlled populations of fleas, ticks, mites and dermatophytes to pose a clinical problem. Minor tick burdens can be removed manually in the clinic, while larger infestations should be killed using a topical acaricide (Table 2). Fly strike, as mentioned above, is always a risk in wild hedgehogs, especially during the summer months. Many cases will require supportive therapy, systemic antibiotics and NSAIDS to aid recovery. Dermatophytosis is the most common infection zoonotically transmitted from hedgehogs to handlers in captivity. Clinical signs are typically apparent in immunocompromised hogs, with alopecia, crusting and pruritus apparent. The treatment of choice is oral antifungal therapy, using terbinafine or itraconazole.3 Prolonged courses of treatment may be necessary. Strict hygiene practices are integral to preventing the spread of infection. Another potential zoonotic agent that has been found in captive wild hedgehogs, is salmonella. Salmonellosis often results in dysentery in juveniles, and outbreaks can occur with high mortality associated. Barrier nursing, fluid therapy, and high dose antibacterial therapy are required for treatment. Most infections are caused by Salmonella Enteritidis PT11 (endemic in hedgehogs), PT66 or Salmonella Typhimurium.6 As there are no drugs licensed for use in hedgehogs, all treatments are given under the cascade. Table 2 outlines the common therapeutic agents and doses used when treating hedgehogs.

Fig 6. Young hoglet.
Euthanasia
Wildlife casualties are very different in their presentation when compared with the domestic species we normally encounter in practice. We can endeavour to save a domestic pet, knowing that a good quality of life is still possible even if they do not return to normal function. This is not always the case for wild animals. From an ethical standpoint, we must only release fully fit animals back into the wild that are capable of sustaining themselves once released. This makes our triage all the more important, as it allows us to assess the viability of the hedgehog from an early stage, and enables us to make the appropriate decision in the interest of the welfare of that individual. There are a number of cases where the decision to euthanise hedgehog casualties should be made: any collapsed and unresponsive patients (the exception to this is hibernating hedgehogs, who may present as unresponsive, but given time and handling should wake); hedgehogs that have sustained an injury that will leave them permanently disabled (eg. amputated limb, comminuted fracture, total blindness, severe respiratory distress from facial injury); severe myiasis; and extensive necrosis of underlying tissues. Senescence can be a cause for euthanasia if end-of-life problems (eg. dental disease, lameness) are inhibiting the hedgehog from carrying out normal behaviours. Euthanasia should be performed by first anaesthetising the patient with gaseous anaesthesia in a chamber or via mask induction. This should be followed by an intracardiac or IV injection (via the cranial vena cava) of pentobarbital. Euthanasia should not be performed without appropriate anaesthesia.
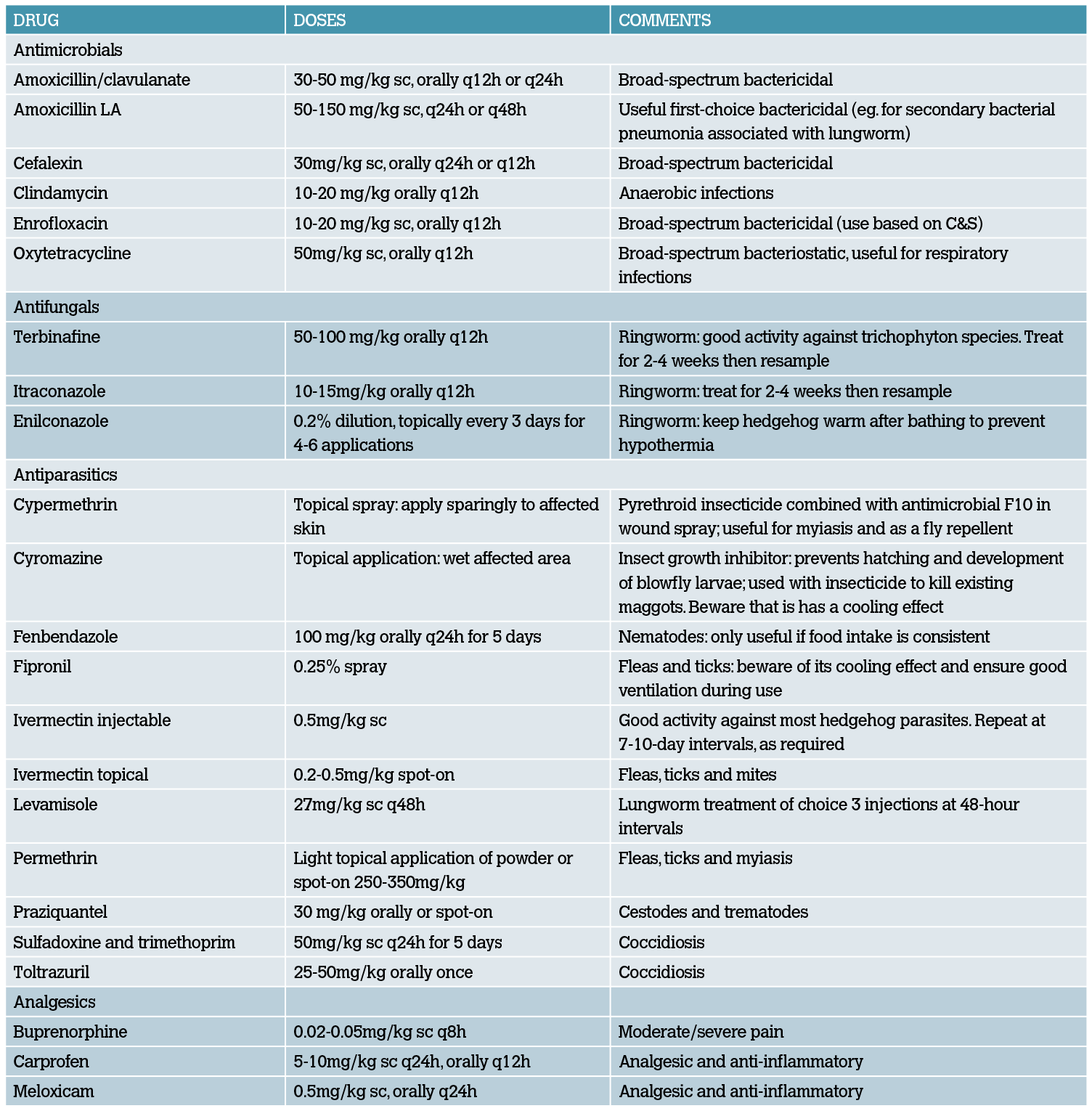
Table 2: Therapeutic agents commonly used in hedgehogs. Adapted from the BSAVA Manual of Wildlife Casualties.
Translocation and release
While the rehabilitated hogs will be released by a trained rehabilitator, it is important that attending veterinarians understand the ultimate goal and expected outcome for these animals. Following the successful rehabilitation of a captive hedgehog, the next step is to release them, close to the site from which they were rescued. If this is not an option, choosing an appropriate habitat, that currently has a resident population of hedgehogs, should be considered. Hedgehogs are not known to be territorial, so releasing them into an already populated location should not pose an issue.8 They should be released at dusk, and away from main roads or urban areas. Hedgehogs kept in captivity for over a month before translocation have been shown to survive longer than those released at an earlier stage.8 As mentioned above, it is vital that underweight hedgehogs are not released in the autumn or winter months. However, it has been shown that healthy rehabilitated hedgehogs, weighing >600g, have been successfully released into the wild during mild spells in the autumn and winter months, with no negative impact on their survival.10 This in turn can reduce the overall time spent in captivity, and limit overcrowding in rehabilitation centres.
Summary
Wildlife cases often appear daunting when presented in general practice. However, if hedgehog casualties are approached in a logical and methodical manner, with the hedgehog’s welfare as your primary focus, they can be extremely rewarding. A basic understanding of the most common injuries and illnesses seen in wild hedgehogs should enable you to provide the best possible care for these enigmatic and endearing little creatures. If you do not feel that your clinic has the capacity to care for a wild hedgehog, there are resources available to help you.
Further information for rehabilitators about juvenile hedgehog body weights for survival during hibernation can be found at www. britishhedgehogs.org.uk/pdf/Hibernation-Weight.pdf
Resources
Wildlife Rehabilitation Ireland run a CVE-accredited two-day wildlife veterinary treatment course every year. To find out more visit their website and join their mailing list for course/conference updates.
-
Bexton S. Hedgehogs. In BSAVA Manual of Wildlife Casualties. 2nd edn. 2016. Eds E. Mullineaux, E. Keeble. BSAVA. pp 117-136.
-
Bexton S, Couper D. Veterinary care of free-living hedgehogs. In Practice 2019; 41(9):420-32.
-
Bexton S, Nelson H. Comparison of two systemic antifungal agents, itraconazole and terbinafine, for the treatment of dermatophytosis in European hedgehogs (Erinaceus europaeus). Vet Dermatol. 2016; 27(6): 500-504.
-
Bunnell T. The Assessment of British Hedgehog (Erinaceus europaeus) Casualties on Arrival and Determination of Optimum Release Weights Using a New Index. Journal of Wildlife Rehabilitation 2002; 25(4): 11-21.
-
Chaprazov, T., Dimitrov, R., Stamatova Yovcheva, K. & Uzunova, K. Oral and dental disorders in pet hedgehogs. Turkish Journal of Veterinary and Animal Sciences. 2014. 38, 1-6.
-
Lawson B., Franklinos, L. H. V., et al. Salmonella Enteritidis ST183: emerging and endemic biotypes affecting western European hedgehogs (Erinaceus europaeus) and people in Great Britain. Scientific Reports. 2018. 8, 1-11
-
Miller EA, ed. Minimum Standards for Wildlife Rehabilitation. 4th edn. 2012. National Wildlife Rehabilitators Association and International Wildlife Rehabilitation Council, St Cloud, MN.
-
Molony SE, Dowding CV, Baker PJ, Cuthill IC et al. The effect of translocation and temporary captivity on wildlife rehabilitation success: an experimental study using European hedgehogs (Erinaceus europaeus). 2006. Biological Conservation 130, 530-537.
-
Robinson, I. Hedgehogs. In Hand-Rearing Wild and Domestic Mammals. Ed L. J. Gage. Iowa State University Press. 2002. pp 75-80.
-
Yarnell RW, Surgery J, Grogan A et al. Should rehabilitated hedgehogs be released in winter? A comparison of survival, nest use and weight change in wild and rescued animals. Eur J Wildl Res 65, 6. 2019.
1. When is it appropriate to see a hedgehog during the day?
A. During the summer months
B. Nursing or pregnant females
C. Young juveniles
D. It is normal for hedgehogs to forage for food during daylight hours
2. What weight should a captive hedgehog reach before releasing them into the wild?
A. >650g
B. >450g
C. >550g
D. >1000g
3. What drug is considered the treatment of choice for Lungworm infection in hedgehogs?
A. Fenbendazole
B. Injectable ivermectin
C. Toltrazuril
D. Levamisole
4. Which of these agents are not of zoonotic risk when handling hedgehogs?
A. Trichophyton erinaceid
B. Salmonella Enteritidis PT11
C. Crenosoma striatum
D. Capillaria aerophila
5. What is the main concern regarding feeding a purely wet food diet to captive hedgehogs?
A. Obesity
B. Nutritional imbalances
C. Dental tartar
D. Anorexia
6. When is it appropriate to keep a wild hedgehog as a pet?
a. If they bond with you while in captivity
B. If they are close to the end of their natural life
C. If they are permanently disabled and cannot be released into the wild
D. It is never appropriate to keep a wild hedgehog as a pet