Ventral midline coeliotomy – reducing post-surgery complications
Fernando S Reina Rodriguez DVM MSc DVMS DipECVS, European specialist in small animal surgery and Professor Barbara Kirby BS RN DVM MS DACVS DECVS American and European specialist in small animal surgery outline how to reduce post-surgical incisional hernia in small animals
Accessing the abdominal cavity using a ventral midline incision is one of the most common surgical approaches in small animal surgery, though the procedure is not free of complications. This article aims to describe risk factors for post-surgical incisional problems to help the reader identify them and avoid those directly influenced by the surgeon, thus keeping the complication rate to a minimum.
Introduction
Ventral midline coeliotomy is one of the most common surgical techniques for abdominal surgery in small animals.1 Most surgeons are very familiar with the approach; it allows rapid access to the abdomen with minimal damage to nerves, vessels and abdominal wall muscles (Figure 1).2
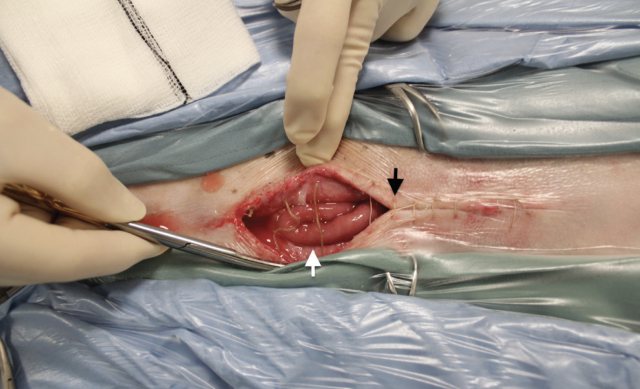
Complications of midline coeliotomy in small animals include surgical-site infection, peritonitis, wound dehiscence, and incisional herniation, which can occur with or without eventration (Figure 2).1
While chronic incisional hernias are commonly associated with patient-dependent factors such as metabolic disease, immunosuppression or development of surgical-site infection,1,3 acute incisional hernias are likely associated with an inadequate surgical technique,1,3,4 inappropriate choice of suture material,1,3 and trauma to the abdominal wall after surgery.5
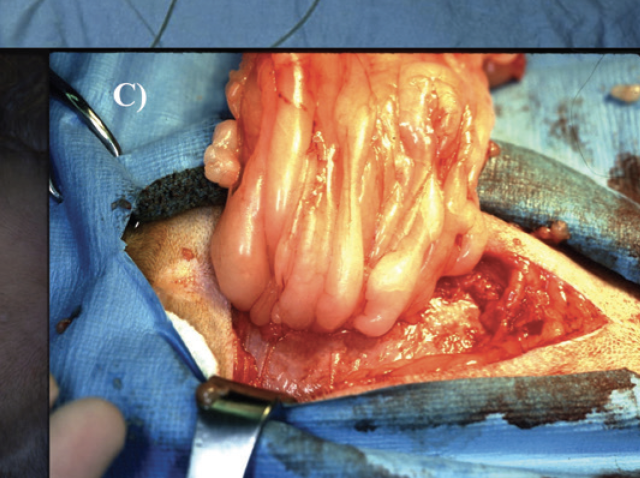
The historical complication rate for midline coeliotomy in small animals, including incisional hernias, appears to be low.6 However, the true incidence is unknown and some authors have suggested it may be underreported,1,7 as suggested by two studies in which a considerable number of patients developed incisional hernias after ovariectomy8 or ovariohysterectomy.5 The consequences of this post-surgical complication, particularly when accompanied by eventration, may be severe (Figure 3).5
The method selected for closure, choice of suture material and the use of an optimal surgical technique are factors under the surgeon’s control that may reduce the complication rate when this approach is chosen.1
Type and length of the surgical incision
In humans, the length and type of incision is considered a risk factor for development of incisional hernia.9,10 Longer incisions are associated with early development of complications,9 while there is an increased risk for open coeliotomy compared to minimally invasive laparoscopic procedures.10 Despite the clear advantages of laparoscopy, incisional hernias can also develop with this technique at either the incisional or the trocar site.10
The type of incision used depends on the anatomic region to expose, type of surgery and the surgeon’s preferences.10 Paramedian incisions provide the theoretic advantage of adding two layers of muscular fascia for closure buttressed by a well-vascularised muscular layer.11 However, paramedian incisions may cause irritation of the tissues included in the closure and postoperative abdominal wall pain.12 In small animals, paramedian incisions are not routinely performed for abdominal surgery because vertical midline incisions provide rapid access to the abdomen.
In humans, transverse incisions have been recommended by some authors because of the lower incidence of incisional herniation and fewer postoperative complications compared to vertical midline incisions.13 However, time required to gain access to the abdomen and to close transverse incisions is generally longer.14 Also, the benefits of transverse incisions for reducing postoperative pain are questionable.15 Transverse abdominal incisions in small animals are reserved for specific procedures such as the flank approach for ovariohysterectomy or the grid approach (small transverse right-paracostal incision) for minimally invasive prophylactic gastropexy.
Surgeon experience and the role of the suture pattern
Independently of the knot configuration or suture material selected, the weakest point in the suture is the knot, followed by the portion of material adjacent to it.16 Slippage of suture material at the knot by inadequate tightening and suture weakening by cramping with the instruments are common mistakes made by inexperienced surgeons. Surgeon’s experience also plays a role in consistent knot security,17 highlighting the importance of forming secure knots during closure.
Simple continuous closure of midline coeliotomy is the standard technique in humans11 as it provides a strong and rapid repair.18 The technique has become accepted in small animals as well.6 However, the amount of tissue to include in the closure, the tension applied in the suture, the distance from the wound edges where the needle is introduced, and the distance between stitches are topics not commonly described in veterinary patients.5-7
In people, the strength of a wound closure using a simple continuous technique depends on the length of suture material used, length of the incision, and the number of stitches used for closure, as determined by the distance between stitches (stitch interval) and the size of the tissue bite (suture bite).19 Assuming that all surgical wounds lengthen about 30% after surgery, the length of suture material used for closure should be at least four times the length of the incision to achieve adequate strength during wound healing.19 Following that rule, the incidence of complications in humans, including incisional herniation, is considerably reduced.2,10,11,18 In small animals, the four-to-one rule is not considered for coeliotomy closure,5-7,20 is not applied or is unconsciously applied by the surgeon.21 This variation between surgeons using a simple continuous technique21 and the fact that incisional hernias are mainly caused by technical errors3 highlights the importance of introducing the four-to-one rule for midline coeliotomy closure in small animals.21
Additionally, reducing the stitch interval and the suture bite have been shown to reduce incisional hernia in humans.18 The suture bite-and-stitch interval in small animals is not reported6,7 or is based on personal experience rather than clinical or experimental studies,20 leaving room for individual interpretation of where and how to place the stitches.
The recommended tension to apply to the suture for closure must be low to prevent compromising blood supply to the local tissue; however, the suture must hold the tissues in apposition while wound healing occurs.22 In areas with relatively low blood supply, such as the linea alba, the suture also needs to retain its strength until the scar tissue can withstand the forces acting on the surgical incision.22
Tissues to include in the closure
Historically, closure of the peritoneum was recommended in humans to prevent herniation because the omentum or a loop of bowel could insinuate into a peritoneal defect, acting as a wedge to enlarge the opening.11 Nevertheless, peritoneal closure was abandoned since it was discovered that peritoneal defects close by cell regeneration23 and the inclusion of peritoneum did not provide additional strength to the closure.24
In dogs, the external leaf of the muscular fascia of the rectus abdominus is the primary strength-holding layer for coeliotomy closure, and no differences are observed compared to full-thickness closure in which the abdominal muscles are included.25 In fact, inclusion of muscle rather than fascia is considered a technical error that may lead to herniation.1 In cats, coeliotomy closure including only the muscular fascia is mechanically comparable to full-thickness closure.26 Fascia-only closure could also reduce postoperative swelling and pain,26 which can increase tension at the incision site after surgery.18
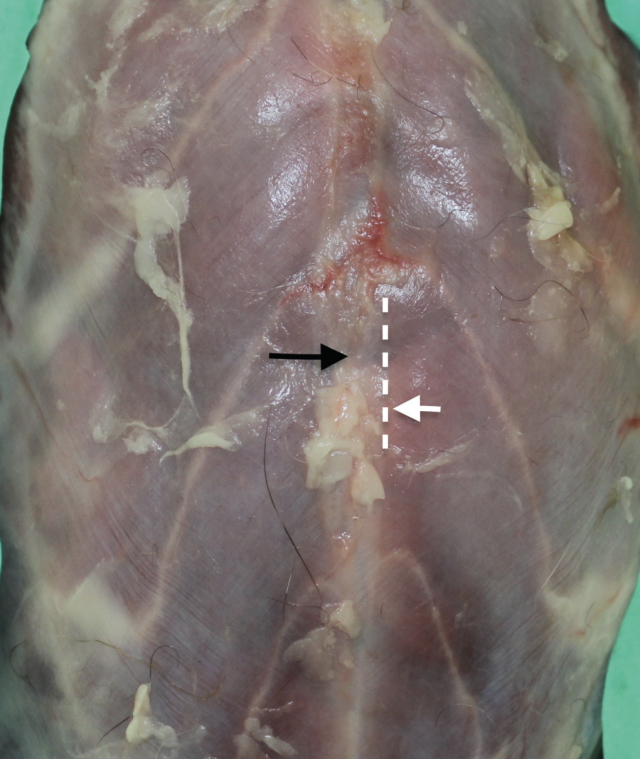
Engaging the muscular fascia during closure involves placing the stitches lateral to the edges of the linea alba. The line limiting the edges of the linea alba and the junction with the fascia of the rectus abdominus is known as the transition zone (Figure 4).27 When sutures are placed here instead of the linea alba, the strength of the closure significantly increases.27
Selection of the suture material and needle
In humans, the ability of scar tissue to withstand forces after a midline coeliotomy incision is about 30% less than that of the intact linea alba.28 This low-resistance capacity may persist for several years after surgery.28 Although similar studies have not been performed in veterinary patients, it is clear that the suture material chosen should provide a secure closure for the duration of wound healing to maintain sufficient strength and ensure tissue apposition until the wound can withstand stress without mechanical support.29
Multifilament materials tend to be stronger and provide better knot security compared to monofilament materials. However, multifilament materials can cause dragging when passed through the tissues leading to suture pull-out and can increase the risk of surgical site infection because of their greater surface area for bacterial penetration.29 Non-absorbable monofilament materials have been recommended in the past,11 but they have been associated with postoperative complications such as persistent postoperative pain and sinus tract.30 Slowly-absorbable monofilament materials are a good choice for coeliotomy closure in humans to avoid the aforementioned complications. In addition, the incidence of incisional hernia is comparable between slowly absorbable and non-absorbable sutures.10,30 Examples of slowly absorbable monofilament materials recommended for coeliotomy closure in small animals include polydioxanone and polyglyconates because of their ability to retain their initial strength for prolonged periods of time.11,29
Suture size selection depends on the patient size, the tissue where it is used and tissue healing ability. Excessively large diameter sutures lead to more foreign material at the surgical site and weaker knot security.11,29 The ideal suture size is the smallest diameter suture that will hold the tissue during wound healing.11 For small dogs and cats, 2 metric (3-0 USP) suture diameter is commonly recommended for coeliotomy closure with the exception of paediatric patients of smaller size, for which 1.5 metric (4-0 USP) may be indicated. For dogs, suture diameter ranges from 3 metric (2-0 USP) to 3.5 metric (0 USP). Larger diameter sutures, such as 4 metric (1 USP), are reserved for giant breeds, where greater forces are expected to occur after surgery at the coeliotomy incision.
Although there are no specific rules for needle selection, an inappropriate needle choice may cause excessive tissue trauma and prolong tissue healing.31 When choosing a needle type, we have to consider the tissue in which the needle will be introduced, the surgeon’s technique, working space and accessibility of the tissue.31 The triangular cutting surface of standard cutting needles facilitates penetration through the tissue; however, the force required to pass the needle may enlarge the suture hole, increasing the risk of suture pull-through.31 The fine point of tapered needles allows for piercing and spreading the tissues during needle passage and is a good option for delicate and easily accessible tissues, such as the ventral abdominal wall.31 The use of curved needles also allows a predictable movement, reducing the force required to penetrate the tissues.31
In humans, the use of a smaller diameter suture and needle size, combined with a simple continuous technique and reducing the stitch interval and suture bite, minimises tissue trauma and reduces the incidence of incisional hernia.18 The effect of needle size and needle type has not been evaluated in small animals, although it seems reasonable to follow the human recommendations.
Conclusion
How to reduce the risk of incisional complications associated with patient-dependent factors?
Incisional hernias are multifactorial in origin. Avoiding the surgical procedure when patient-dependent factors are identified is not a reasonable solution. Nevertheless, it is important, not only to recognise patient-dependent factors, but also to minimise their impact on the occurrence of complications. Adequate treatment of pre-existing metabolic diseases, such as diabetes or hyperadrenocorticism, appropriate surgical planning and selecting a minimally invasive approach when possible are some of the measures to take when surgery is required in these patients.
Which surgical approach do I use for abdominal surgery?
With few exceptions, vertical midline incision through the linea alba is the standard and preferred technique. The length of the incision will vary depending on the procedure, exposure required and the surgeon’s experience. When possible, and particularly in high-risk patients in which wound healing may be compromised, reducing the incision length or selecting a minimally invasive procedure should be considered.
How to close midline coeliotomies?
Select a slowly absorbable monofilament material of adequate diameter and the smallest and least traumatic needle. Then, use a simple, continuous technique including only the external leaf of the fascia of the rectus abdominus. This is the accepted technique in humans and small animals. Apply enough tension during closure to appose the wound edges without compressing the tissues to avoid impairment of the local blood supply. Ideally, do not include muscle during closure to reduce postsurgical pain and swelling.
What number of stitches do I have to use?
The number of stitches will depend on the length of the incision. The length of suture material used for closure should be at least four times the length of the incision. Surgeons must consider the four-to-one rule to ensure adequate strength of the surgical wound, particularly during the initial phases of wound healing.
Where to place the stitches?
The needle must penetrate the external leaf of the fascia of the rectus abdominus. This involves placing stitches at the transition zone, lateral to the edges of the linea alba and the junction with the fascia of the rectus abdominus. This area should be identified prior to coeliotomy closure.
- De Rooster H. Celiotomy. In: Complications in Small Animal Surgery. Griffon D, Hamaide A. 1st ed. Wiley-Blackwell. Hoboken, New Jersey; 2016: 355-361
- Harlaar JJ, Deerenberg EB, van Ramshorst GH et al. A multicenter randomized controlled trial evaluating the effect of small stitches on the incidence of incisional hernia in midline incisions. BMC Surgery 2011; 11: 20-27
- Smeak DD (1993). Abdominal hernias. In: Disease Mechanisms in Small Animal Surgery. Bojrab MJ. 2nd ed. Lippincott Williams and Wilkins, Philadelphia; 2019: pp 98-102
- Claeys S. Dehiscence. In: Complications in Small Animal Surgery. Griffon D, Hamaide A. 1st ed. Wiley-Blackwell. Hoboken, New Jersey; 2016: pp 57-63
- Gower SB, Weisse CW, Brown DC. Major abdominal evisceration injuries in dogs and cats. J Am Vet Med Assoc 2009; 234: 1566-1572
- Crowe DT. Closure of abdominal incisions using a continuous polypropylene suture: clinical experience in 550 dogs and cats. Vet Surg 1978; 7: 74-77
- Boothe HW, Skater MR, Hobson HP et al. Exploratory celiotomy in 200 non-traumatized dogs and cats. Vet Surg 1992; 21: 452-457
- Charlesworh TM, Sanchez FT. A comparison of the rates of postoperative complications between dogs undergoing laparoscopic and open ovariectomy. J Small Anim. Pract 2019; 60: 218-222
- Veljkovic R, Protic M, Gluhovic A et al. Prospective clinical trial of factors predicting the early development of incisional hernia after midline laparotomy. J Am Coll Surg 2010; 210: 210-219
- Le Huu Nho R, Mege D, Ouaïssi M, et al. Incidence and prevention of ventral incisional hernia. J Visc Surg 2012; 149: e3-e14
- Poole GV (1985). Mechanical factors in abdominal wound closure: the prevention of fascial dehiscence. Surgery 1985; 97: 631-639
- Suleiman MD, Johnston DE). The abdominal wall: an overlooked source of pain. Am Fam. Physician 2001; 64: 431-438
- Grantcharov TP, Rosenberg J. Vertical compared with transverse incisions in abdominal surgery. Eur J Surg 2001; 167: 260-267
- Inaba T, Okinaga K, Fukushima R et al. Prospective randomized study of two laparotomy incisions for gastrectomy: midline incision versus transverse incision. Gastric Cancer 2004; 7: 167-171
- Halm JA, Lip H, Schmitz PI, et al. Incisional hernia after upper abdominal surgery: a randomized controlled trial of midline versus transverse incision. Hernia 2009; 13: 275-280
- Von Fraunhofer JA, Chu CC. Mechanical properties. In: Wound Closure Biomaterials and Devices. CRC Press, Boston, Massachussets; 1996: pp 121-128
- Marturello DM, Mc Fadden MS, Bennet RA et al. Knot security and tensile strength of suture materials. Vet Surg 2014; 43: 73-79
- Israelsson LA, MIllbourn D. Prevention of incisional hernias: how to close a midline incision. Surg Clin North Am 2013; 93: 1027-1040
- Jenkins TP. The burst abdominal wound: a mechanical approach. Br J of Surg 1976; 63: 873-876
- Bellenger CR. Abdominal wall. In: Textbook of Small Animal Surgery. Slatter DH. 2nd ed. Saunders, Philadelphia; 1993: pp 405- 413
- Degasperi B, Klonner ME, Dupre G. Evaluation of suture length to wound length (SL:WL) ratio in an in vitro abdominal closure model. Scientific Presentation Abstracts: European College Veterinary Surgeons, 25th Annual Scientific Meeting 2056; pp 22
- Langley-Hobbs SJ. Sutures and general surgical implants. In: Feline Soft Tissue and General Surgery. Langley-Hobbs, SJ, Demetriou JL, Ladlow JF. Saunders, Philadelphia; 2014: pp 105-107
- Hubbard TB, Khan MZ, Carag VR et al. The pathology of peritoneal repair: its relation to the formation of adhesions. Ann Surg 1967; 165: 908-916
- Gurusamy KS, Cassar Delia E, Davidson BR. Peritoneal closure versus no peritoneal closure for patients undergoing non-obstetric abdominal operations. Cochrane Database Syst Rev 2013; 4: CD010424
- Rosin E, Richardson S. Effect of fascial closure technique on strength of healing abdominal incision in the dog: a biomechanical study. Vet Surg 1987; 16: 269-272
- Reina Rodriguez FS, Buckley CT, Milgram J, Kirby BM. Biomechanical properties of feline ventral abdominal wall and celiotomy closure techniques. Vet Surg 2018; 47: 193-203
- Tera H, Aberg C. Tissue strength of structures involved in musculo-aponeurotic layer sutures in laparotomy incisions. Acta Chir Scand; 142: 349-355
- Hollinsky C, Sandberg S. Measurement of the tensile strength of the ventral abdominal wall in comparison with scar tissue. Clin Biomech 2007; 22: 88-92
- Boothe H. Selecting suture materials for small animal surgery. Compend Contin Educ Vet 1998; 20: 155-161
- Van’t Riet M, Steverberg EW, Nellenteyn J et al. Meta- analysis of techniques for closure of midline abdominal incisions. Br J Surg 2002; 89: 1350-1356
- Scmiedt CW. Suture material, tissue staplers, ligation devices and closure methods. In: Veterinary Surgery Small Animal. Tobias and Jonhston. 1st ed. Elsevier. St Louis, Missouri; 2012: pp 180-191
1. Which of the following statements is true?
a Chronic incisional hernias are commonly caused by surgeon-related factors
b Acute incisional hernias only occur if the patient performs vigorous exercise during the immediate postoperative period
c Acute incisional hernias may be associated with poor surgical technique, inappropriate selection of suture material or trauma during the postoperative period
d Chronic incisional hernias may be associated with poor surgical technique, inappropriate selection of suture material or trauma during the postoperative period
2. You have to perform an exploratory coeliotomy on a patient with hipoproteinaemia. The pre-operative diagnosis is unclear. You want to make the most of your surgery from the diagnostic point of view, so you may consider obtaining biopsies from different organs. Which surgical approach would you use?
a Ventral midline coeliotomy. I would try to slightly reduce the length of my incision without affecting the adequate visualisation of the abdominal organs
b Ventral right paramedian incision. The two-layer muscle closure will reduce the chances of a chronic incisional hernia due to hipoproteinaemia
c Ventral left paramedian incision. The two-layer muscle closure will reduce the chances of a chronic incisional hernia due to hipoproteinaemia
d Right or left paracostal incision
3. The four-to-one rule should be applied for
a Longer incisions, particularly in high risk patients
b Paramedian incisions
c Paracostal incisions
d All of the above. This rule must be used to increase the mechanical strength of our wound closure, particularly during the initial phases of wound healing
4. You have to perform an exploratory coeliotomy on a patient diagnosed with septic peritonitis. Which suture material would you use to close the abdominal wall?
a Non-absorbable multifilament material as the pre- existing infection may slow the wound healing
b Non-absorbable monofilament material
c Long-lasting absorbable multifilament material
c Long-lasting absorbable monofilament material
5. You have finished an abdominal surgery on a 2kg Chihuahua. Which suture material would you use to close your coeliotomy?
a 0 USP polydioxanone
b 0 USP polyglyconate
c 3/0 USP polydioxanone or 3/0 USP polyglyconate
d 2/0 non-absorbable material, such as nylon or polypropylene
Answers: 1:C; 2:A; 3:D; 4:D; 5:C.