Ensuring clinic and personnel biosecurity in an equine hospital: developing an infection control policy
In this article, Samantha Feighery BSc (Hons) RVN, Rossdales LLP outline ways to implement infection control and biosecurity policies and protocols for your practice and details the different components that a basic biosecurity plan should contain, for example preventative measures hygiene, staff training, protective clothing, barrier nursing and isolation protocols
The main aim of an infection-control programme is to implement the biosecurity protocols, to manage and reduce the introduction of contagious organisms within the hospital, and to reduce infection risks, including infections that are hospital acquired (Burgess et al, 2014). It also is designed to prevent inpatients from acquiring infections and provide treatment and supportive care to infected patients or patients who are suspected to have a contagious disease.
Clinic/hospital biosecurity plan
It is important that a practice has a biosecurity plan in place that is easily available to all employees. All new staff members should receive training in the infection-control protocols employed by the clinic and how they affect their individual roles; for example, yard staff in managing the movement of patients, or the receptionist recognising clinical signs that need to be referred to a vet before admission to the clinic, eg. loose feces/nasal discharge.
The biosecurity plan should detail strict hygiene protocols for all staff members, the method of cleaning and disinfection of hospital equipment and the entire facility. It provides guidelines on how to stable horses according to infection-risk groups, for example day patients and hospitalised patients stabled in different parts of the yard.
Ideally, a staff member would be responsible for maintaining logs/records of stables/paddocks where potentially/confirmed infectious patients were housed. These records facilitate future audits and help identify biosecurity failures or successes. A plan helps put a policy in place to ensure continuing staff education and training, this applies to all areas of the team, from reception, yard staff and all veterinary personnel. For example, in the case of an outbreak like the equine flu this year, all staff at this author’s facility were trained in a new policy for admitting patients to the hospital. This involved the use of protective clothing, a smock, gloves and taking the patient’s temperature prior to admission.
Appointment of infection control officers, particularly in a large practice, is essential to ensure implementation of and adherence to the infection control protocols that were devised. In larger clinics, it may be recommended to have a representative from different departments, eg. a vet, vet nurse and yard staff. The responsibilities of the infection control officers are to ensure biosecurity guidelines and procedures are adhered to, to encourage all staff members to contribute to infection control, and to provide in-house training to all staff on biosecurity and infection control policies.
Components of biosecurity plan
The first component of a biosecurity plan is putting preventative measures in place to minimise risk.
Separation of patients by risk
- Detection of high-risk patients early is vital. Specific measures need to be used in order to detect high-risk patients early, for example receptionists refer all cases with clinical signs of diarrhoea or neurological signs or certain respiratory signs to the veterinary surgeon in charge to consent to referral. This means the owners can be instructed to unload the horse directly at the isolation stables thereby reducing the risk of the horse coming into any contact with other horses in the car park.
- Patients are divided into risk categories according to their infectious disease status. Day patients and poor performance patients are generally low-risk category whereas a sick post-operative colic patient would be a higher risk category. Ideally, these patients are not housed in close contact. A useful protocol to use is tags with a designated colour on the front of the stable to communicate the infectious status of the animal to all staff. For example, a lowest-risk category is a green tag generally, indicating patients with ringworm. Orange tags are generally for sick foals and indicate discharging wounds.
- The highest-risk categories, eg. horses with acute diarrhoea, strangles, EHV1, should be housed in the separation/isolation unit away from main yard.
- Sick adults, and post-op colic surgery patients are barrier-nursed (Figure 1) in an adult intensive care unit (ICU). There is evidence to show that equine colic patients are at high-risk of developing various types of infections and shedding enteric organisms, eg. salmonella species (Burgess & Morley, 2014).
- Sick neonatal foals and mares are barrier nursed in neonatal intensive care unit (NICU).
Hygiene
- Hand hygiene is the most important defense against the transmission of disease within an equine hospital. Many studies show that there is a link between good hand-hygiene policies and the concurrent reductions in hospital acquired infections (Verwilghen, 2018) so it’s important in a veterinary hospital or clinic that a high standard is maintained. It is recommended to wear gloves and wash hands before and after touching each patient.
- Effective cleaning and disinfection are essential in preventing the transmission of infectious pathogens between patients or staff or from contaminated equipment and environments.
- It is the responsibility of all staff members to maintain hospital cleanliness and appropriate personal hygiene.
- Uniforms and suitable footwear (dependent on area of work) should always be worn. Ideally, staff change their uniforms at work (in particular the staff directly dealing with patients) and the uniforms are laundered at the hospital.
- Daily cleaning with appropriate disinfectant of all clinical and reception areas is mandatory or as needed, for example cleaning holding boxes after bandage changes especially after contaminated wounds.
Protective clothing and barrier nursing
- Its important to have a protocol in place to assist in deciding which patient should be placed in barrier nursing or isolation, and when. This needs to be easy to access for all staff, particularly if the clinic/hospital admits patients out of hours.
- For example, in this author’s hospital, all patients in the adult and neonatal ICU are automatically barrier nursed. These entails gloves and smocks/overalls being worn and a footbath is placed outside the stable.
Staff training
- All staff should receive training on:
- Use of personal protective equipment;
- The importance of good hand hygiene. Use of signage at hand-washing sinks demonstrating the correct method of hand washing is useful;
- The correct concentrations of disinfectant to be used. Again, signs with instructions on or around the bottles/dispenser are useful; and
- All staff educated on zoonotic and contagious diseases of importance and their routes of transmission, eg. salmonella, strangles, MRSA.
- Isolation protocols
- All staff, particularly personnel admitting patients, must be aware of what qualifies a patient to be admitted to isolation. It is important to train reception staff to recognise some clinical signs that would lead them to refer the admission to a vet/vet nurse.
- Having a summary of this protocol in a central location that is easily accessible is recommended for ease of reference. For example, a folder in the nurse’s station and online on the intranet.
An example of an isolation admitting protocol is:
- Patients are admitted to isolation if some following is present:
- Acute diarrhoea;
- Leucopenia;
- Pyrexia; or
- Known to have strangles/abortigenic EHV1/MRSA/neurological signs consistent with EHV1/exotic disease/dystocia/fever with or without respiratory signs.
Other environmental controls
- Rodent and vector control: entry portals are sealed, eliminate clutter and sources of standing water, animal food is stored in closed metal or thick plastic containers. Food waste is disposed of properly to keep the facility free of rodents, house flies and other arthropods.
- Eating and drinking should only to be done in designated areas. These activities should never be done in animal-care areas or in the laboratory. Do not keep food or drink for human consumption in the same refrigerator as equine food, biologics, or laboratory specimens.
- Use of paddocks by patients should be recorded and used in a manner that reduces infection risk. This may be recorded a spreadsheet or simply a note pad.
Cleaning and disinfectant protocol
- Surfaces cannot be disinfected properly if they are not clean. All organic material (bedding/manure) must be removed before cleaning. Scrubbing of surfaces plays an important role in removing biofilms and stubborn stains, especially in stables and holding boxes.
- Follow instructions on products for correct dilutions, uses, contact time, disposal and whether wearing personal protective equipment (PPE) is required with each disinfectant.
- All boxes are emptied/cleared, steam cleaned with appropriate disinfectant, left to dry, fogged with another disinfectant. The advantage/purpose of fogging is to create and disperse a disinfectant aerosol to reduce the numbers of airborne micro-organisms and also to apply disinfectant to surfaces that may be difficult to reach.
Environmental swabbing
- After the stable has been cleaned, disinfected and fogged, it is left to dry.
- Once dry, environmental swabs are taken and sent to the lab for culture. PPE is worn while taking these swabs.
- The case type or diagnosis will determine the swab protocol, eg. if the patient had salmonella the stable would not be used again until three sets of swabs came back negative. And swab three is not taken until day 11 post cleaning and disinfecting.
Monitoring and audits
- Regular monitoring and performing audits lets us assess if our policies are effective, which enables the practice to ensure continuous improvement.
- Monitoring of the whole hospital environment ensures frequent cleaning and disinfection of all areas.
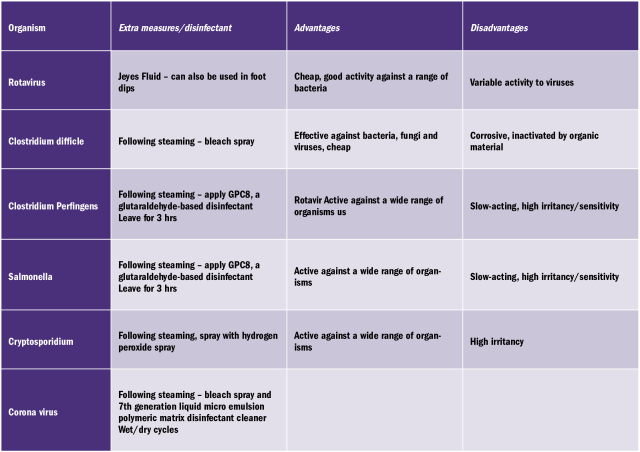
- To facilitate ease of monitoring, details of the patient’s barrier nursed on the main yards and patients admitted to the isolation unit can be recorded in separate logbook. If the pathogen has been identified, this is also recorded and this will determine which disinfectant is most appropriate for example if the patient is found to have rotavirus, the stable will be cleaned with Jeyes fluid.
- Demonstrates how effective the cleaning and disinfection protocols are working.
- Disadvantage is that it is expensive.
- Holding bi-annual an infection-control meeting with all staff is an opportunity to evaluate the practices protocols and their effectiveness. Its an opportunity to discuss failings or ways to improve. All staff are invited, this is an opportunity to evaluate the practices protocols, their effectiveness and discuss failings or ways to improve.
Summary
In summary, biosecurity and infection control is every staff member’s responsibility. It’s important to implement nursing, cleaning and disinfecting practices that will reduce the burden of contamination in your facility, eg. good hand hygiene amongst staff.
-
Lane, C. 2016, "Preventing surgical site infections: equine surgical site preparation", The Veterinary Nurse, vol. 7, no. 3, pp. 151-155.
-
McMillan, S. 2014, "An evidence-based approach to infection control in the operating theatre", The Veterinary Nurse, vol. 5, no. 4, pp. 194-200.
-
Sprayberry, K.A. & Robinson, N.E. 2015, Robinson's current therapy in equine medicine, Seventh / [ by] Kim. A. Sprayberry, N. Robinson. edn, Elsevier Saunders, St. Louis, Missouri
-
Verwilghen, D. 2018, "The World Health Organization's Clean Hands Save Lives: A concept applicable to equine medicine as Clean Hands Save Horses", Equine Veterinary Education, vol. 30, no. 10, pp. 549-557.
-
Burgess, B.A. & Morley, P.S. 2014, "Infection Control in Equine Critical Care Settings", Veterinary Clinics of North America: Equine Practice, vol. 30, no. 2, pp. 467-474.
-
Rebecca Bevan . (2010). Effective approaches to barrier nursing and controlling infection. Vet Times. Nov (1), 2.
-
Pittet, D., Hugonnet, S., Harbarth, S., Mourouga, P., Sauvan, V., Touveneau, S. & Perneger, T.V. 2000, "Effectiveness of a hospital-wide programme to improve compliance with hand hygiene", The Lancet, vol. 356, no. 9238, pp. 1307-1312.